https://meditropics.com/?page_id=904&preview=true
*Harshita Singh
*Post Graduate resident, Lady Hardinge Medical College, New Delhi
A 51-years old farmer from Rewari district of Haryana, India had complaints of decrease in appetite, weight loss (20kg in past 6 months), generalized myalgia and fatigue, salt cravings, mild abdominal discomfort and darkening of skin for past 6 months. He had no known co-morbidities, and no history of travel, no significant past history but had a history of alcohol, tobacco and hukkah smoking. Family history was insignificant.
On examination, patient had a GCS = E4V5M6, pulse rate of 88/min, BP= 98/60mmHg, RBS= 105cmg/dl and was maintaining a saturation of 98% on room air. Hyper-pigmentation could be appreciated on the sun exposed areas, palmar creases and tongue (Figure 1). No pallor, icterus, clubbing, cyanosis, lymphadenopathy or edema was noticed. Systemic examination was within normal limits.

He was worked up for the above-mentioned complaints. Laboratory investigations were suggestive of mild anemia, hyponatremia, hyperkalemia, normal TSH and ESR = 44 mm/hr. Serum cortisol level was on the lower side (76.2nmol/L).
HIV status was non-reactive. Chest X-ray was grossly normal. Patient had HbA1c of 7% and was diagnosed as a case of Type 2 Diabetes Mellitus, although was not compliant with the treatment.
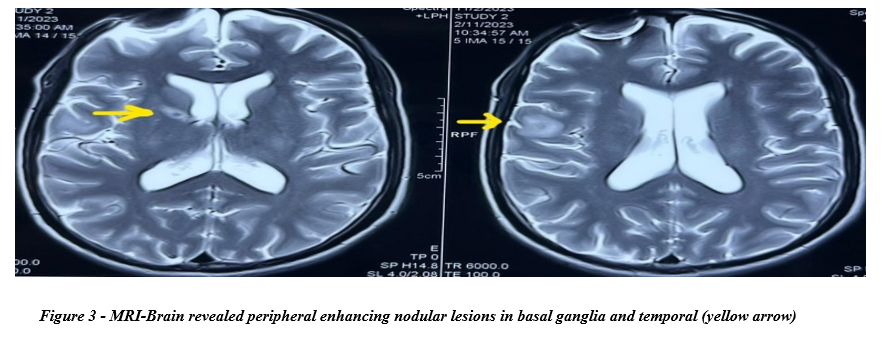
PET-CT shows FDG avid lymph nodes in cervical region. Also, both adrenal SOLs show patchy abnormal FDG uptake (Figure 2). MRI-Brain revealed peripheral enhancing nodular lesions in basal ganglia and temporal (Figure 3).
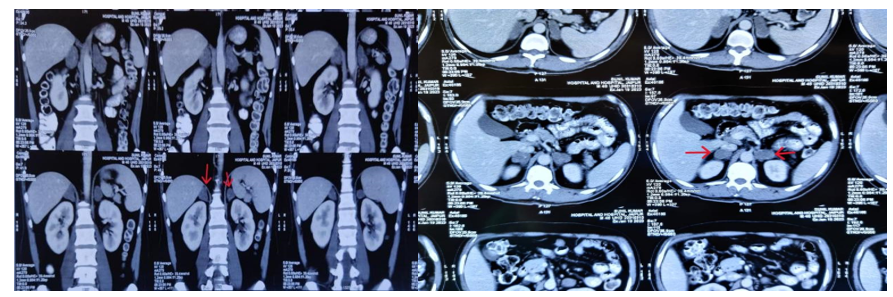
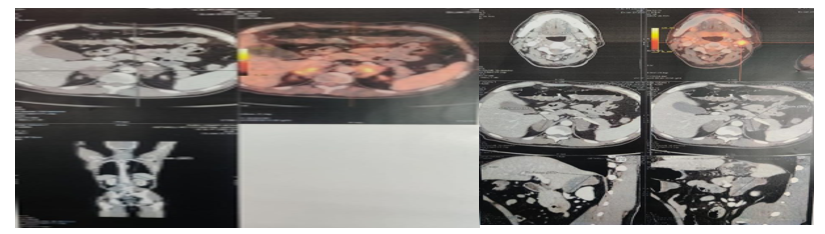
Figure 2 – Mildly enhancing, hypodense SOL, symmetrically involving bilateral adrenal glands (red arrows).
DIFFERENTIAL DIAGNOSIS:
Based on history, examination, labs and radiological findings, a diagnosis of Type 2 Diabetes Mellitus with Primary Adrenal Insufficiency was made, and following differentials were kept
- Tuberculosis
- Malignancy (Primary or metastasis)
- Infections (Meningococcal, fungal infections)
BIOPSY LEADING TO A DEFINITIVE DIAGNOSIS!
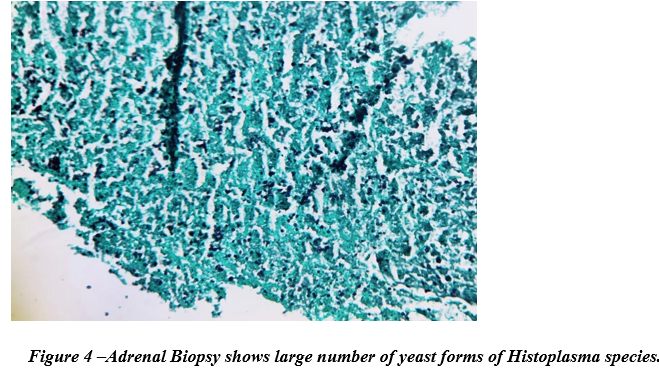
A CT- guided biopsy was performed from the one of adrenal lesions and sent for histopathological examination. HPE showed large number of yeast forms of Histoplasma species (Figure 4 – Gomori Methenamine silver stain was positive).
FINAL DIAGNOSIS:
Thus, a final diagnosis of Progressive disseminated histoplasmosis with primary adrenal insufficiency was made.
TREATMENT
The patient was started on lyophilized Amphotericin-B(1mg/kg/day) for 28 days, oral glucocorticoids and mineralocorticoids. He was then shifted on Itraconazole 200mg BD and discharged with resolution of symptoms.