ANTI-RO52 POSITIVE AMYOPATHIC DERMATOMYOSITIS WITH UNDERLYING LUNG CANCER
Harshita Umesh1, Latika Gupta2
1Bangalore Medical College and Research Institute, Bangalore, Karnataka, India
2Department Clinical Immunology and Rheumatology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India
https://meditropics.com/pc-2022-2/
ABSTRACT:
The association of Dermatomyositis (DM) with cancer is well-established. However, certain features like autoimmunity, interstitial lung disease, and arthritis may signify an autoimmune than paraneoplastic cause with negative predictive value for malignancies. We discuss the case of a 54- year old lady with amyopathic DM with arthritis and anti-Ro52 positivity where age and significant weight loss were the only silent pointers to an underlying lung adenocarcinoma. It is imperative for physicians to carefully look for clinical clues and conduct age-appropriate screening for cancer in patients diagnosed with DM for timely management.
KEYWORDS: Dermatomyositis, inflammatory polyarthritis, Anti- Ro52, amyopathic dermatomyositis, lung adenocarcinoma
PRESENTATION:
A 54-year-old lady presented to the rheumatologist with inflammatory polyarthritis involving the small joints of the hands for the past six months. She also reported fever, myalgia and significant weight loss over the same duration.
On examination, she had tenderness of the proximal interphalangeal joints and wrists with a positive squeeze sign. Edema and erythema of the eyelids were noted, prompting a suspicion of a heliotrope rash in the setting of inflammatory myositis (Figure 1). Gottron’s papules and shawl sign was seen. On auscultation, fine inspiratory crepitations were heard in the left infrascapular area suggesting a possibility of underlying interstitial lung disease.

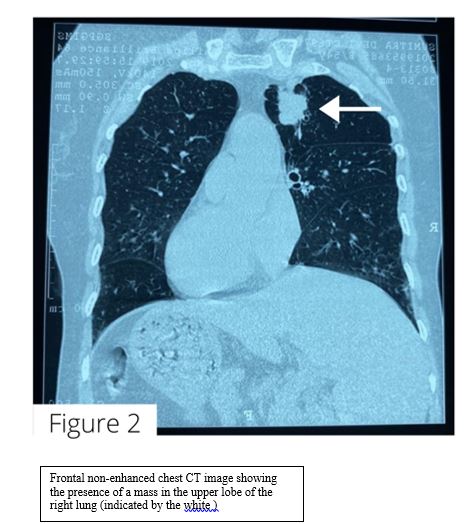
Anti-Ro52 was positive on Myositis antibody testing. Surprisingly, a chest CT (Figures 2) revealed a mass with speculated margins in the right upper lobe instead, with lung adenocarcinoma confirmed later with histopathology. A diagnosis of cancer associated dermatomyositis was made.
DISCUSSION:
The association of cancer with DM is well-established with an incidence varying from less than 7% to over 30% [1] , while the incidence of the occurrence of DM in lung cancer is approximately 10%[2] of those with cancer. However, certain clinical features when associated with DM, such as interstitial lung diseases (ILD), arthritis, and anti-Ro52 carry negative predictive value for underlying cancer. Certain myositis-specific autoantibodies such as anti-TIF1γ, on the other hand, carry a positive predictive value.[3] Although amyopathic DM such as in this patient is thought to be associated with cancer associated myositis, this association has been refuted in recent literature.
In this case, the patient presented with myositis along with autoimmune features like arthritis and anti-Ro52 antibodies which may connote a better prognosis and absence of underlying cancer. Clinical examination also suggested crepitations which serve as red herrings for ILD but led to an incidental diagnosis of cancer instead.
It is noteworthy that she reported significant weight loss, a red flag which mandates age-appropriate screening for malignancy. This report highlights that clinical signs such as age and weight loss and a careful clinical examination mandate high index of suspicion for cancer, even when the presentation is not classic. While standard guidelines on cancer screening in myositis are still underway, it is imperative for clinicians to maintain a key index of suspicion with simple clinical clues such as older age, male gender, significant weight loss, refractory and early dysphagia, angry red rash on the hairline, and refractory ulcers for timely diagnosis of cancer associated DM 4] This could go a long way in improving the survival of DM patients with malignancies.
REFERENCES:
- Di DR, Abeni D, Tracanna M, Capo A, Amerio P: Cancer risk in dermatomyositis: a systematic review of the literature. G Ital Dermatol Venereol. 2014, 149:525-37.
- Kanaji N, Watanabe N, Kita N, Bandoh S, Tadokoro A, Ishii T, Dobashi H, Matsunaga T. Paraneoplastic syndromes associated with lung cancer. World J Clin Oncol. 2014 Aug 10;5(3):197-223. doi: 10.5306/wjcov5.i3.197. PMID: 25114839; PMCID: PMC4127595.
- Gupta L, Naveen R, Gaur P, Agarwal V, Aggarwal R (2021) Myositis-specific and myositis-associated autoantibodies in a large Indian cohort of inflammatory myositis. Semin Arthritis Rheum 51(1):113–120
- Oldroyd AGS, Allard AB, Callen JP, Chinoy H, Chung L, Fiorentino D, George MD, Gordon P, Kolstad K, Kurtzman DJB, Machado PM, McHugh NJ, Postolova A, Selva-O’Callaghan A, Schmidt J, Tansley S, Vleugels RA, Werth VP, Aggarwal R. A Systematic Review and Meta-Analysis to Inform Cancer Screening Guidelines in Idiopathic Inflammatory Myopathies. Rheumatology (Oxford). 2021 Feb 18 keab166. doi: 10.1093/rheumatology/keab166. Epub ahead of print. PMID: 33599244.
ADDRESS FOR CORRESPONDENCE
.Latika Gupta
Assistant Professor
Department of Clinical Immunology and Rheumatology
Sanjay Gandhi Postgraduate Institute of Medical Sciences
Lucknow, India
Email: drlatikagupta@gmail.com
Phone number: 05222495182