Classic Raymond Syndrome: A Rare Ventral Pontine Stroke
Atul Goel(1) , Aanchal Arora (2), Monika Tanwar(3), Subodh Kumar Mahto(4), Sanjay Kumar Meena(5)
(1) Director Professor and Head of the Unit, Department of Medicine, LHMC Hospital, New Delhi
(2) Assistant Professor, Department of Medicine, LHMC and RML Hospital, New Delhi
(3) Assistant Professor, Department of Medicine, ABVIMS and RML Hospital, New Delhi
(4) Senior Resident, Department of Medicine, ABVIMS and RML Hospital, New Delhi
(5) Junior Resident, Department of Medicine, ABVIMS and RML Hospital, New Delhi
(2) Corresponding Author : aanchal7565@gmail.com
ABSTRACT
Raymond syndrome is a pontine stroke due to lesion in paramedian pons. Among the two types Classic and Common type, the latter is commonly seen. Classic type is rare and only few cases have been reported in the past. We report the case of a 52 year old diabetic and hypertensive gentleman presenting with left sided hemiplegia, ipsilateral upper motor neurone type facial palsy and contralateral abducenspalsy. Brain imaging revealed a right sided subacute infarct in the mid-pons. Hence the presence of a right sided mid-pontine infarct with contralateral hemiplegia, contralateral upper motor neurone facial palsy and ipsilateral abducent nerve palsy validated the entity of Classic Raymond syndrome.
KEYWORDS
Ventral Pontine stroke, Classic Raymond Syndrome, corticofacial fibres
INTRODUCTION
Raymond Syndrome (Ventral pontine stroke) is a rare posterior circulation stroke in the ventral medial caudal pons as a result of affection of the paramedian branches of the basilar artery. Literature describes two subtypes of Raymond Syndrome namely Common and Classic type, former being reported the most. These delineated types of syndromes are explained on the basis of the intricate neuroanatomical network of fibres in the pons. In the ventral caudal pons, corticofacial fibres, corticospinal tract and the abducent nerve fascicle are arranged medial to lateral respectively. The corticofacial fibres and corticospinal tracts decussate at the level of upper medulla. In the Common Raymond Syndrome the vascular lesion affects the undecussated corticospinal fibres, abducent nerve but spares the corticofacial fibres. This presents as contralateral hemiplegia with ipsilateral abducent nerve paralysis without facial nerve involvement. Whereas in Classic type the vascular lesion extends medially to also affect the undecussated corticofacial fibres. Raymond syndrome is also known as alternating abducens hemiplegia.
CASE REPORT
A 52 year old gentleman, right handed presented to our hospital with sudden onset weakness of left side of body and slurring of speech for one day. He noticed the weakness when he woke up in the morning which involved the left upper and lower limb simultaneously and was complete at onset. He was unable to articulate clearly and experienced double vision on looking towards right side. His attendants also noticed facial asymmetry and drooling of secretions from left side of the face. He also complained of headache which was diffuse and holocranial. There was no history of fever, loss of consciousness, convulsions, vomiting or neck pain. He denied any associated chest pain, shortness of breath, palpitations or syncope. He was diagnosed with type II diabetes mellitus and hypertension and was taking indigenous medicines irregularly. He was an active smoker and used to consume alcohol occasionally, though he denied any binge intake prior to admission. He denied any history of similar episode in the past, coronary artery disease, seizure disorder and thyroid disorder. On general physical examination, he was conscious and oriented to time, place and person. His pulse was 76 / minute, regular and blood pressure was raised to 170/80 mm Hg in the right arm in supine position. He was afebrile and was maintaining saturation upto 99% at room air by pulse oximetry. There was no evidence of pallor, icterus, clubbing, cyanosis, lymphadenopathy and pedal edema on examination. Jugular venous pressure was not raised.
A thorough neurological examination revealed a Glasgow Coma Scale (GCS) of 11/15 (E4V5M2). Speech was comprehensive but slow and slurred. There was facial asymmetry, deviated angle of mouth towards the right and flattened nasolabial fold on the left side. Muscles of forehead were spared and bell’s phenomenon was absent. Thus left sided upper motor neuron type facial palsy was present (Figure 1). There was restriction of right eye movement and diplopia in right lateral gaze indicating right sided sixth nerve palsy. Pupillary size and reaction was normal bilaterally. Other cranial nerves were normal. Motor examination revealed grade 2/5 power in left upper limb and lower limb at all joints. Tone was normal in both upper and lower limbs bilaterally. Muscle bulk was comparable on both sides in all limbs. No abnormal and involuntary movements were observed in any part of the body. Gait could not be assessed due to unilateral weakness. Deep tendon reflexes (biceps, triceps, supinator, knee and ankle jerks) were brisk on left side and normal on right side. Babinski sign was present on left side while plantar reflex was flexor on right side. Superficial abdominal reflex was absent on left side. All primary sensory modalities were intact on face, limbs and trunk. No signs of meningeal irritation and raised ICT were observed. Right sided cerebellar function was intact while left sided could not be assessed. Fundus examination was normal. Rest systemic examination was unremarkable.

Figure 1
A diagnosis of stroke (right sided pontine infarct) with contralateral hemiplegia, facial paresis and ipsilateral abducent nerve palsy with type II diabetes mellitus and hypertension was made. Haematological and biochemical parameterswere essentially normal except deranged blood glucose levels and lipid profile (Table 1). Electrocardiogram (ECG) showed left ventricular strain hypertrophy with strain. Chest Radiograph had cardiomegaly. Non contrast computed tomogram (NCCT) of the brain revealed acute infarct in right sided pons (23 HU hypodensity) and mild age related atrophy changes. Ultrasonography of the abdomen showed grade I fatty liver. 2D echocardiography was suggestive of mild concentric left ventricular hypertrophy with ejection fraction of 55%. Contrast Enhanced Magnetic Resonance Imaging (CEMRI) of the brain showed involved area to be hyperintense on T2 with few blooming foci, suggestive of subacute infarct with bleed in right half of pons (Figure 2). MR angiography brain was normal. Patient was managed conservatively with anti platelet therapy, statin, anti hypertensives, oral hypoglycemic agents and short acting insulin to achieve target blood glucose levels between 140-180 mg/dL. Appropriate physiotherapy and symptomatic treatment was given. He was discharged thereafter a stay for 10 days to follow up in outpatient department. Three months later he had near complete recovery of the neurological limb and cranial nerve weakness.
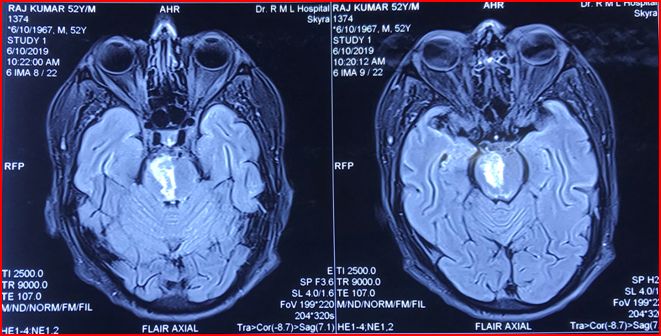
Figure 2
Table 1 : Laboratory Parameters at Day 1
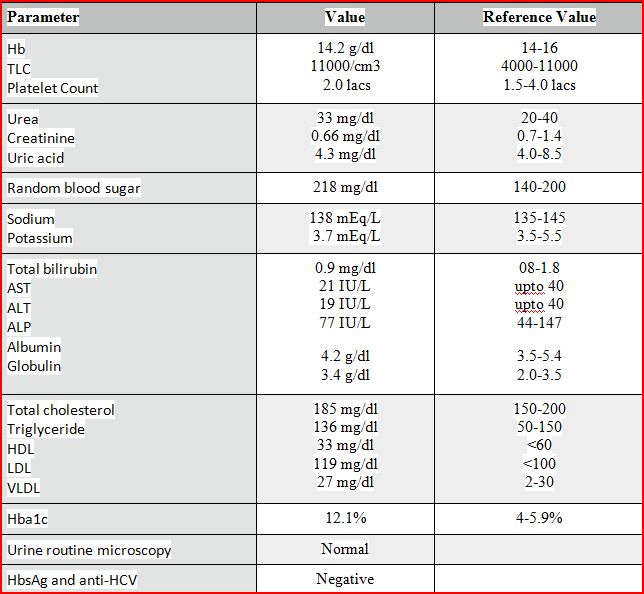
(Abbreviations- Hb: Haemoglobin, TLC: Total Leucocyte Count, AST: Aspartate Transaminase, ALT: Alanine Transaminase, ALP: Alkaline Phosphatase, HDL: High Density Lipoprotein, LDL: Low Density Lipoprotein, VLDL: Very Low Density Lipoprotein)
DISCUSSION
Classic Raymond Syndrome is an extremely rare entity presenting as contralateral hemiplegia and central facial paresis with ipsilateral abducent nerve palsy. An important differential of Ventral Medial Pontine stroke is Millard Gubler syndrome which presents as ipsilateral peripheral facial and abducens nerve palsy and contralateral hemiparesis [1]. This syndrome affects the base of the ventral pons to affect the facial and abducent nerve fascicles. The paramedian branches of the basilar artery supply the caudal medial pons (abducent nerve and nucleus, corticospinal and corticofacial fibres). Occlusion of the vascular supply to these structures which are arranged in an intricate manner manifests as Classic and Common Raymond Syndrome (Figure 3a,3b).
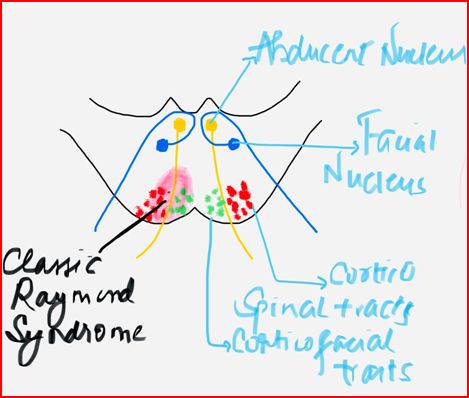
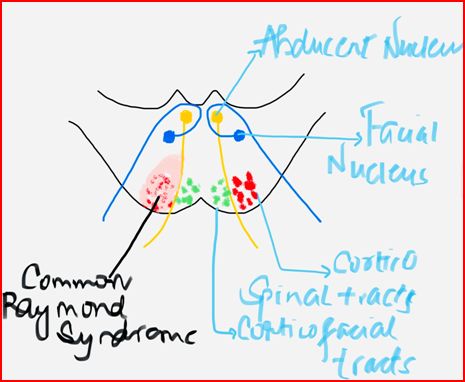
Figure 3a Figure 3b
Classic Raymond syndrome was described by French neurologist Fulgence Raymond in 1896 in a syphilitic woman who presented clinically with left sided abducens nerve palsy and right sided hemiparesis along with UMN type facial nerve palsy [2]. Raymond hypothesised the presence of contralateral facial paresis due to affection of facial fibres just before their decussation in caudal pons. However this observation was refuted by further case reports [3,4] of caudal medial pontine stroke with ipsilateral abducent nerve palsy and alternating hemiplegia without facial involvement, thereafter described as Common Raymond Syndrome.
Classic Raymond Syndrome entity was further validated by Sheth and colleagues in 1996 in a 55 year old female with infarct in left medial caudal pons [5]. In 2012 ZaorskyNG and Luo JJ also reported a case of 50 year old man with right sided abducent impairment and contralateral hemiparesis and central facial paresis due to subacute infarct in right medial caudal pons [6]. They validated the Classic Raymond Syndrome and proposed the concept of both Classic and Common type. Worldwide very few case reports of similar presentation have been published among which Khan et al [7] in 2017 reported the first case from South Asia. We report the case of Classic Raymond Syndrome in a 52 year old gentleman with uncontrolled hypertension, diabetes mellitus and hyperlipidemia.
CONCLUSION
This case reminds us of an unusually seen ventral Pontine stroke. Hence we as clinicians should keep this syndrome in mind whenever a case of alternating abducent hemiplegia is encountered.
REFERENCES
- Yasuda Y, Matsuda I, Sakagami T, Kobayashi H, Kameyama M. Pontine infarction with pure Millard-Gubler syndrome: precise localization with magnetic resonance imaging. European neurology. 1993;33(4):333-4.
- Raymond F. Leçons Sur Les Maladies Nerveuses. 1894–1895. Paris, France: Ire Ser, Ricklin & Soques; 1896. Concerning a special type of alternating hemiplegia; 365–383.
- Ogawa K, Suzuki Y, Kamei S. Two patients with abducens nerve palsy and crossed hemiplegia (Raymond syndrome) Acta Neurologica Belgica. 2010;110(3):270–271.
- Satake M, Kira JI, Yamada T, Kobayashi T. Raymond syndrome (alternating abducent hemiplegia) caused by a small haematoma at the medial pontomedullary junction. Journal of Neurology Neurosurgery and Psychiatry. 1995;58.
- Sheth RD, Riggs JE, Ortiz OA. Raymond syndrome: a validation. European neurology. 1996;36(3):173- 4.
- Zaorsky NG, Luo JJ. A case of classic raymond syndrome. Case Rep Neurol Med. 2012;2012:583123.Khan M, Naveed S, Haider I, Humayun M, Khan A. Classic Raymond Syndrome. J Coll Physicians Surg Pak. 2017 Mar;27(3):185-2012;2012:583123.
- Khan M, Naveed S, Haider I, Humayun M, Khan A. Classic Raymond Syndrome. J Coll Physicians Surg Pak. 2017 Mar;27(3):185-186.