Acute onset breathlessness in a patient on anti-tuberculous therapy- emphysema or pneumothorax
PICTORIAL CME
Vipin Dev(¹), Rashmi Rajput(²), Shivraj Meena(³), Riya Samanta(⁴), Bhawna Satija(⁵)
(¹)Junior Resident, Department of Medicine, Lady Hardinge Medical College, New Delhi
(²)Senior Resident, Department of Medicine, Lady Hardinge Medical College, New Delhi
(³)Associate Professor, Department of Medicine, Lady Hardinge Medical College, New Delhi
(⁴)Senior Resident, Department of Radiology, Lady Hardinge Medical College, New Delhi
(⁵)Associate Professor, Department of Radiology, Lady Hardinge Medical College, New Delhi
A 30-year male, chronic smoker, driver by occupation, was diagnosed 2 months back as reactivation of pulmonary tuberculosis on basis of symptoms of fever, weight loss, appetite loss and chest radiography. Patient was started on anti-tubercular treatment (ATT) 2 months back, but now he presented to Medicine emergency with history of acute breathlessness for 1 day. Examination of the respiratory system revealed fullness of intercostal spaces and reduced chest wall movement on the right side with a hyper-resonant percussion note, and reduced breath sounds. Chest X-ray of the patient was performed (Figure 1). What does it show?
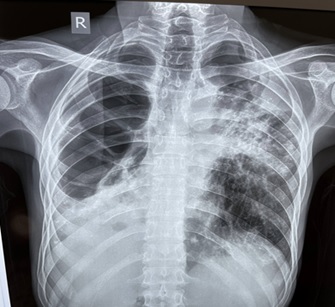
Figure 1- Chest- X ray of the patient.
The chest X-ray of the patient (Figure 1) shows a centrally placed trachea with lobulated hyperlucent areas (without lung markings with curvilinear margin)-red arrows, in Right Upper zone and middle zone with fibrotic bands, suggestive of emphysematous bullae. An inhomogeneous opacity is seen in right lower zone, which could be a consolidated right lower lobe with areas of breakdown. An area of lucency is seen in left upper zone, multiple fibronodular opacities in left middle and lower zone, with pulled up left hilum and tenting of left diaphragm.
In this case, the presenting history and clinical examination was suggestive of right sided pneumothorax. However, chest-X ray showed bullae on a background of sequalae of old infection (tubercular) with some areas of active infection. Presence of hyperlucent area with curvilinear margin points towards bulla, whereas in pneumothorax margins of hyperlucent area are usually regular. However, it may, at times be difficult to distinguish these two entities on chest-X ray. CECT chest (Figure 2) further cleared the diagnosis and pneumothorax was ruled out. Hyperlucent areas on X-ray corresponded to areas of thick-walled cavity. Patient was managed conservatively and was discharged on ATT.
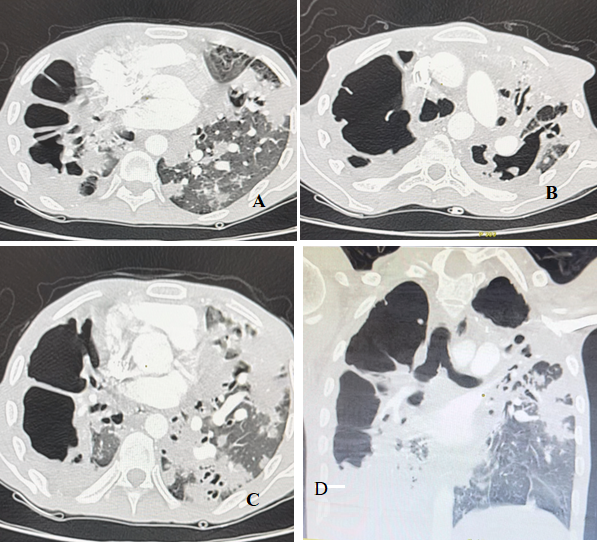
Figure 2 – CECT chest
Figure 2- CECT chest showed multiple large thick-walled cavities involving almost all segments of right lung as well as left upper lobe (red arrows) with almost complete destruction of right lung and left upper lobe. Areas of fibro atelectatic and bronchiectatic changes involving basal segments of RLL and left upper lobe, suggestive of old tubercular changes. Centrilobular tree in bud nodules with few of them coalescing to form patches of consolidation with areas of breakdown within noted involving basal segments of left lower lobe suggestive of active infective etiology likely reactivation of pulmonary tuberculosis.
Though the clinical history and examination often provide a straightforward diagnosis of pneumothorax, it is necessary to obtain an imaging and look for red flag signs before making a diagnosis of pneumothorax. An intercostal drain insertion should be done only when the diagnosis has been confirmed.