https://meditropics.com/1193-2/
*Abhishek Ranjan, **Anupam Prakash,*** Shubha Laxmi Margekar
*Post-graduate Resident, Lady Hardinge Medical College, New Delhi
**Director Professor, Lady Hardinge Medical College, New Delhi
***Professor ,Lady Hardinge Medical College, New Delhi
ABSTRACT: Dengue is a tropical infection with varied presentation and bleeding from various sites can be a fatal complication. Pleural effusion because of capillary leak is quite common in Dengue Fever. Rarely, it can cause hemothorax. We report a case of a young woman, who presented with high grade fever, myalgia, and fatigue and generalised weakness for 5 days. During hospital stay, she developed pleural effusion. IgM and IgG Dengue were positive. Diagnostic thoracocentesis for the same yielded blood. CT Angiography didn’t reveal any bleeding vessels. Urgent tube thoracostomy was done along with supportive management. Her clinical symptoms improved gradually and ICDs were removed after 5 days. This is the rare case of bilateral massive hemothorax in a patient of dengue in India.
INTRODUCTION: Dengue fever is caused by a ssRNA virus from Flaviviridae family. It has four serotypes which are designated as DENV1-4. Globally as much as 100-400 million infections are occurring each year with around 25% people producing symptoms. Based on global modelled data, an estimated 33 million clinically apparent Dengue cases occur in India each year, contributing to a third of the total global disease burden. [1] Dengue can be clinically classified into three subgroups: Dengue Fever, Dengue Hemorrhagic Fever and Dengue Shock Syndrome. Hemorrhagic Dengue usually manifests as mucocutaneous bleed, rarely it can present with hemothorax.
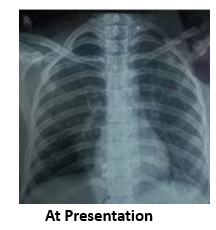
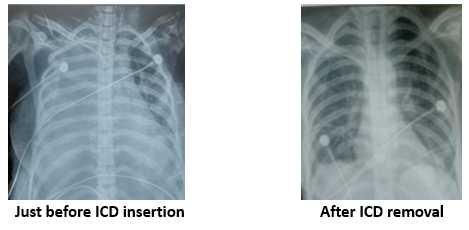
CASE SUMMARY: A 28-year-old hypothyroid female presented with history of high grade fever associated with chills, myalgia, and retro-orbital pain for 5 days. On presentation, patient was in shock and had to be put on inotropes. Her pulse rate was 118/min, Spo2 98% on room air, temperature was 102°F. Systemic examinations were normal. Initially there was no history of bleeding from any site. During the critical phase, she developed respiratory distress. Chest X-ray revealed bilateral massive pleural effusion. A diagnostic pleural tap yielded blood on both sides. Haematocrit of pleural fluid was >50% of that of venous blood. Ascitic tap was also done and the fluid was blood tinged. Urgent inter-costal drainage (ICD) tubes insertion was done and around 2 Litres of blood was drained on right side and 1.5Litres on left side within 24 hours. Fresh frozen plasma and packed red blood cells were transfused. Patient improved symptomatically and over a period of 3-4 days, ICD output decreased and ICDs were ultimately removed.
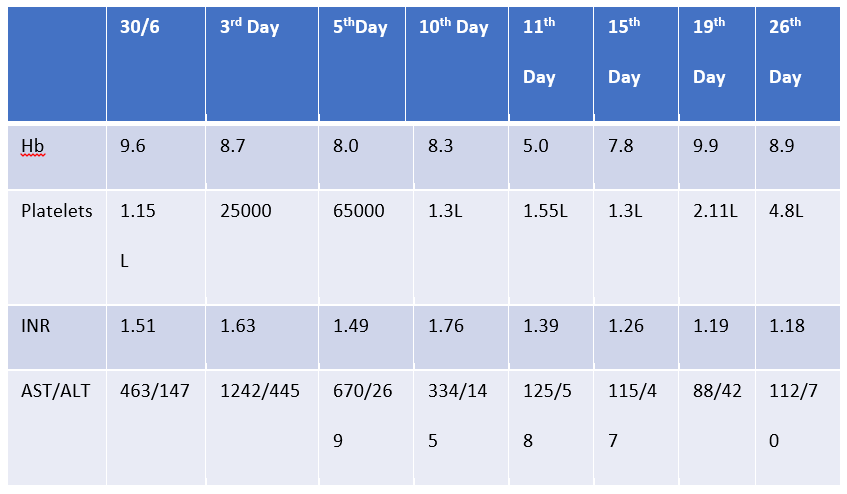
Investigations Revealed-IgM Dengue: Positive on Day 8 of illness (NS1 –ve), Malaria Card test – Negative, Hepatitis A/B/C/E – Negative, Scrub Typhus and Leptospira tests were negative, Blood Culture: Sterile, X-ray (Day 4 of admission) – Homogeneous Opacity over bilateral lung fields, USG whole abdomen suggestive of – Moderate ascites with pseudo–Gall bladder wall edema, CECT Chest + CT Angiography: Bilateral pleural effusion with collapsed lungs. No bleeding vessels, ECG- Low voltage complexes. 2D Echocardiography was suggestive of mild pericardial effusion with ejection fraction 25-30%. Pleural fluid analysis showed – Protein – 1.46g/dL (Serum protein- 5.8), LDH – 363 (Serum LDH – 1564)
DISCUSSION: Severity and nature of the dengue virus is influenced mainly by genetic variability, age and immune status of the host. [2] The ability of all DENV serotypes to utilize pre-existing heterotypic flavivirus antibody to enhance infection is a unique feature of DENV and is considered to be the primary basis of DENV pathogenesis. Respiratory manifestations in Dengue fever are pulmonary edema, ARDS, pulmonary hemorrhage and pleural effusion. Bleeding in dengue infection is multifactorial including defects in coagulation cascade, platelet dysfunction, DIC and thrombocytopenia. Treatment of hemothorax in dengue includes achieving and maintaining hemodynamically stability followed by urgent tube thoracostomy and administration of blood products. A thoracotomy may be needed in case of incessant bleeding into the ICD tube.A similar case was reported in Mumbai by Chirag Aggrawal et al in which a middle-aged male presented as unilateral hemothorax as a complication of Dengue. [2]Patient was managed conservatively and improved gradually. Similarly, unilateral haemothorax was noted by Karanth SS et al., but in this case haemothorax was massive and it required intercostal drainage. [3]
CONCLUSION: Dengue infection is a great masquerader. It’s presentation ranges from mild fever to life threatening bleeding manifestations including hemothorax. Especially in endemic areas like Delhi, doctors need to be aware that a non-traumatic hemothorax can be a manifestation of dengue hemorrhagic fever. So that timely intervention can help in better outcome of patient.
REFERENCES:
- WHO. Dengue: Guidelines for diagnosis, treatment, prevention and control. New edition. Geneva: World Health Organization; 2009.
- Agrawal L C, Tuteja HS. Haemothorax, an Unusual Presentation in Dengue: A Case Report. Journal of Clinical & Diagnostic Research. 2021 Jul 1;15(7).
- Karanth SS, Gupta A, Prabhu M. Unilateral massive hemothorax in Dengue hemorrhagic fever: A unique presentation. Asian Pac J Trop Med. 2012;5(9):753- 54.